

If you’re considering spinal mobilisation, it’s crucial to watch for red flags that could point to serious underlying conditions. These warning signs help identify when manual therapy might be unsafe or when immediate medical attention is required. Here’s a quick rundown:
- History of cancer: Past cancers, especially those likely to spread to bone, can weaken the spine and make mobilisation risky.
- Unexplained night pain or neurological symptoms: Persistent night pain, leg weakness, or changes in bladder/bowel function could signal nerve or spinal cord issues.
- Recent trauma or fracture risk: Falls, accidents, or conditions like osteoporosis can increase the risk of spinal fractures.
- Signs of infection or systemic illness: Fever, chills, or a history of intravenous drug use may indicate spinal infections.
- Vascular symptoms: Dizziness, vision problems, or difficulty speaking during neck movements could suggest blood flow issues in the cervical spine.
Each of these red flags requires careful evaluation, often involving imaging or interest in referrals, to ensure patient safety and avoid complications.
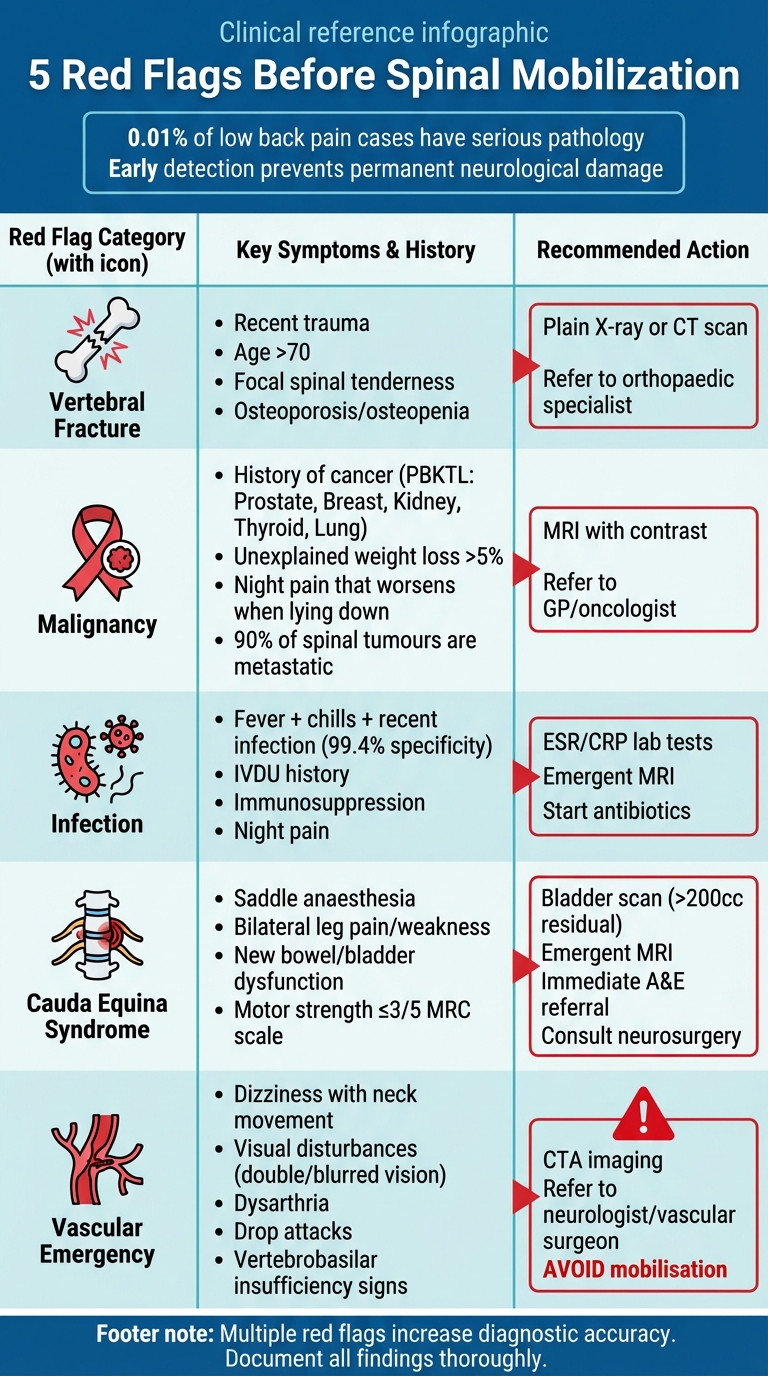
5 Red Flags Before Spinal Mobilization: Warning Signs and Actions
5 minute Physio tip – Contraindications and red flags to cervical spine manual therapy
sbb-itb-585d67d
Red Flag 1: History of Cancer
When evaluating back pain, a history of cancer deserves close attention. Around 90% of spinal tumours are metastatic, and vertebral metastases appear in approximately 10% of newly diagnosed cancers. Even when a patient is in remission, undetected metastatic lesions can compromise spinal stability, especially during treatment.
To remember the primary cancers most likely to spread to bone, use the mnemonic "PBKTL": Prostate, Breast, Kidney, Thyroid, and Lung. In women, breast and lung cancers account for nearly 80% of skeletal metastases, while in men, prostate and lung cancers make up a similar percentage of cases. Multiple myeloma, the most common primary bone tumour in adults, often affects the spine and can result in vertebral compression fractures.
Symptoms to Watch For
Certain symptoms may point to metastatic involvement. Pain that worsens when lying down is a hallmark of vertebral metastasis, unlike degenerative pain, which typically eases with rest. Other warning signs include unexplained weight loss exceeding 5% within four weeks, persistent thoracic spine pain, or pain that remains constant throughout the day and night.
"Back pain is the initial feature of spinal cord neoplastic disease in about 90% of adult patients." – Jesse Borke, MD, FACEP, FAAEM
Neurological symptoms like leg weakness, numbness, or changes in bowel and bladder function may indicate spinal cord compression. Interestingly, pain often appears two to four months before other symptoms of cord compression, offering a critical window for early detection.
What Practitioners Should Do
When these red flags are present, advanced imaging, such as an MRI with contrast, should be considered before manual therapy. Plain X-rays are generally inadequate because osteolytic lesions only become visible after 30% to 50% of bone mineral loss.
A thorough case history is essential, focusing on night pain, unexplained weight loss, and any new neurological symptoms. If concerns arise, practitioners, such as a chiropractor in Sydney, should work closely with the patient’s oncologist or GP to rule out active metastatic disease before proceeding with spinal mobilisation or other treatments.
Red Flag 2: Unexplained Night Pain or Neurological Deficits
When it comes to patient safety, this red flag points to signs that could indicate serious neurological issues. Persistent night pain is a key concern here. Unlike mechanical back pain, which usually eases with rest, unexplained night pain might point to conditions like spinal cord compression or infection. If this symptom is paired with worsening neurological issues, immediate medical attention is essential. Here’s how to spot these red flags and act quickly.
How to Recognise the Signs
Certain symptoms can signal nerve compression or other serious problems. For instance:
- Bilateral leg pain combined with changes in urinary, bowel, or sexual function. Ask patients about trouble urinating, loss of bowel control, or altered sensation.
- Saddle anaesthesia (numbness in the perianal or perineal area) is a classic sign of cauda equina syndrome.
- Bilateral motor weakness can suggest spinal cord or nerve root compression. A motor strength of 3/5 on the MRC scale should raise concerns.
While physical tests like assessing anal tone are unreliable, a thorough patient history is crucial for identifying these issues.
"Diagnosis and treatment of the CESS (Suspected) and the CESI (Incomplete) patient will achieve the best outcomes but these are the patients where clinical assessment has poor predictive value. Therefore all patients whose diagnosis is ‘? CES’ (including the CESS patient with bilateral radiculopathy) require urgent MRI." – Nick Todd
When to Refer
The presence of these symptoms demands swift action. Patients showing bilateral leg pain with CES symptoms – like saddle anaesthesia, bladder or bowel dysfunction, or sensory changes – should be sent immediately to A&E for an emergency MRI.
For patients with bilateral leg pain and worsening neurological signs, even without CES symptoms, an urgent MRI should be arranged within a week. If bilateral leg pain is present but neurology is intact and no CES symptoms are observed, it’s important to provide clear "safety netting" instructions. Patients should be advised to seek emergency care if their symptoms worsen. When in doubt, referring early can help avoid permanent neurological damage.
Red Flag 3: Recent Trauma or Fracture Risk
Recent trauma could point to vertebral fractures, which make spinal mobilisation unsafe. Missing a fracture diagnosis can lead to severe consequences, including permanent neurological damage or even death. This risk is especially concerning in specific trauma situations, as outlined below.
Common Scenarios
Trauma from falls, car accidents, or sports injuries often raises concerns, but it’s also crucial to think about patients with conditions like osteoporosis or osteopenia. These individuals can experience fractures from seemingly minor incidents, like a stumble or an awkward twist. When trauma is combined with an age over 70, there’s a 98.7% specificity for identifying vertebral fractures – meaning fractures are highly likely in these cases. However, sensitivity is just 5.2%, indicating that fractures can still happen in younger patients or without clear trauma. These considerations highlight the importance of thorough risk evaluation before attempting mobilisation.
"The challenge for clinicians is to quickly identify patients with a serious spinal pathology that contraindicates manipulative therapy or necessitates immediate referral to a medical interest in." – Ronald Feise, DC
Precautionary Steps
As with other red flags, taking a detailed patient history is critical. Enquire about recent falls, accidents, or impacts, and assess for risk factors such as long-term corticosteroid use, smoking, or diagnosed osteoporosis. During the physical exam, tapping on the spinous processes can help identify areas of tenderness that might signal a fracture. For older patients reporting trauma, plain X-rays should be performed before considering mobilisation. In more complex cases – particularly where ligament damage or spinal canal issues are suspected – a CT scan may be necessary. If a fracture is suspected or confirmed, avoid manual therapy and refer the patient immediately to an orthopaedic or neurosurgical interest in.
Red Flag 4: Signs of Infection or Systemic Illness
Spinal infections are extremely uncommon (around 0.01% of low back pain cases), but they can imitate mechanical issues and carry serious risks. Identifying these infections often requires a detailed patient history and careful examination before considering spinal mobilisation. Detecting these infections early can be tricky, as symptoms are often subtle or even absent. When an infection is confirmed, spinal mobilisation is not an option due to the potential for permanent neurological damage.
Symptoms to Monitor
Be on the lookout for a combination of symptoms such as fever, chills or sweating, and a recent infection. Together, these symptoms are highly specific for spinal infections, with a specificity rate of 99.4% when all three are present. However, the sensitivity is only 7.5%, meaning many patients with an infection may not show this complete set of signs.
Certain patient histories can raise the level of concern. For example, individuals with immunosuppression (due to HIV, long-term corticosteroid use, or recent surgery), intravenous drug use, or tuberculosis are at higher risk of spinal infections like discitis. Systemic signs to watch for include general malaise, an increased pulse rate, or localised symptoms such as redness, heat, or swelling near the spine. Additionally, sudden, severe spinal pain without a traumatic cause – or a noticeable change in the usual pain pattern, especially if it worsens at night – should prompt further investigation.
These signs and symptoms demand urgent attention and action.
Steps to Take
Quickly recognising the signs of a spinal infection is critical. If a patient presents with fever, chills, and a recent infection, they should be referred immediately for diagnostic evaluation. Spinal infections rule out manipulative therapy, and any delay in diagnosis can lead to irreversible damage.
"The challenge for clinicians is to quickly identify patients with a serious spinal pathology that contraindicates manipulative therapy or necessitates immediate referral to a medical interest in." – Ronald Feise, DC
For cases involving unusual or persistent pain that don’t meet all the criteria, it’s essential to keep monitoring the patient closely and maintain communication with their medical doctor. Since red flag screenings often have low sensitivity, the absence of symptoms doesn’t guarantee the absence of an infection. Staying alert and cautious across all red flags ensures the safety of your practice and your patients.
Red Flag 5: Vascular or Vertebrobasilar Symptoms
Issues with blood flow in the cervical spine can pose serious risks, especially during spinal mobilisation. The vertebral artery, which passes through the cervical spine, is responsible for supplying blood to critical areas like the brain stem and cerebellum. When this blood flow is disrupted – a condition known as vertebrobasilar insufficiency – the results can be devastating, potentially causing lasting neurological damage or even death.
High-Risk Indicators
Certain symptoms can signal vertebrobasilar insufficiency. Watch for dizziness or vertigo that occurs with neck movements. Visual problems, such as double vision, blurred vision, or temporary vision loss, are also key warning signs. Other symptoms to be aware of include difficulty speaking (dysarthria), trouble swallowing, sudden loss of balance, or unexpected drop attacks.
Pay close attention if these symptoms are linked to neck rotation or extension. For instance, if a patient reports feeling dizzy when turning their head, this could suggest vascular involvement. The presence of multiple symptoms like these should raise concern and warrant additional investigation.
Clinical Response
If vascular or vertebrobasilar symptoms are present, avoid spinal mobilisation entirely. As one expert highlights:
"Neck manipulation should be done gently with care to avoid excessive rotation that could damage the patient’s vertebral artery." – Quackwatch
In such cases, it’s essential to refer the patient for further evaluation. This might involve advanced imaging techniques like Computed Tomography Angiography (CTA) or a consultation with a neurologist or vascular surgeon. Be sure to document all symptoms thoroughly and make appropriate referrals without delay. While red-flag screening is often highly specific, it’s not always sensitive, so ongoing vigilance is crucial even if initial assessments seem clear.
Clinical Checklist for Spinal Mobilisation Safety
Checklist Overview
To ensure safe and effective spinal mobilisation, clinicians should use a systematic checklist to screen for critical conditions such as vertebral fractures, malignancies, infections, cauda equina syndrome, and vascular emergencies. This process helps in making informed clinical decisions.
Here’s a quick summary of key red flags, associated symptoms, and recommended actions:
| Red Flag Category | Key Symptoms & History | Recommended Action |
|---|---|---|
| Vertebral Fracture | Trauma, age over 70, focal spinal tenderness, osteopenia/osteoporosis | Perform a plain X-ray or CT scan; consult an orthopaedic interest in |
| Malignancy | History of cancer, unexplained weight loss, night pain or sweats | Order an MRI; refer to a GP or oncologist |
| Infection | Fever, chills, history of intravenous drug use (IVDU), recent surgery, immunodeficiency | Conduct ESR/CRP lab tests, perform an emergent MRI, and start antibiotics |
| Cauda Equina | Saddle anaesthesia, new bowel or bladder dysfunction, bilateral leg weakness | Use a bladder scan (check for >200cc residual), perform an emergent MRI, and consult neurosurgery |
| Vascular Emergency | Pulsatile abdominal mass, history of AAA or hypertension | Perform a point-of-care ultrasound (POCUS); order a CTA for stable patients and consult vascular surgery immediately |
Combining multiple red flags, such as a history of cancer and unexplained weight loss, can improve diagnostic accuracy. This checklist aligns with the systematic screening approach mentioned earlier.
Importance of Documentation
Thorough documentation is just as essential as the screening itself. Record both the presence and absence of red flags to establish a baseline, track any changes, and support your clinical decisions. This meticulous approach not only ensures patient safety but also provides a clear record of your reasoning.
"The challenge for clinicians is to quickly identify patients with a serious spinal pathology that contraindicates manipulative therapy or necessitates immediate referral to a medical interest in." – Ronald Feise, DC
Good documentation also facilitates communication with other healthcare professionals. By including a detailed history, examination findings, and any discussions with the patient’s GP, you create a transparent and collaborative record. This is crucial, especially considering that while over 80% of patients in primary care may present with at least one red flag, fewer than 1% are ultimately diagnosed with a serious condition.
Conclusion
Why Vigilance Matters
Screening for potential warning signs before spinal mobilisation is an essential step in protecting patients from serious harm. Although severe conditions like vertebral fractures (0.7% to 4.0% of cases), malignancy (0.0% to 0.2%), spinal infection (0.01%), and cauda equina syndrome (0.04%) are rare, missing these diagnoses can have devastating consequences. A delay in identifying these issues can lead to permanent neurological damage.
"Early diagnosis of these pathologies is vital, because a missed or delayed diagnosis can lead to permanent harms such as severe, irreversible neurological compromise or death." – Ronald Feise, DC
The difficulty lies in the fact that individual red flags often lack sensitivity. This makes it crucial to assess multiple indicators together and track any changes in symptoms over time. For instance, combining unexplained weight loss with a history of cancer provides a 99.8% specificity, while trauma in patients over 70 years old has a 98.7% specificity. These combinations significantly improve diagnostic accuracy. Additionally, incorporating insights from other healthcare professionals into the evaluation process further enhances the safety and effectiveness of care.
Working with Other Healthcare Providers
Beyond thorough screening, collaboration with other healthcare providers is key. If red flags are identified, it’s essential to refer the patient to a medical interest in immediately to rule out serious conditions. This team-based approach ensures patients receive well-rounded care tailored to their individual needs.
Clear communication with the patient’s GP is especially important in complex cases where symptoms persist or new concerns arise. A collaborative system helps ensure all healthcare providers are aligned in their understanding of the patient’s condition. By sharing clinical findings and coordinating care, practitioners can address serious conditions promptly while continuing safe musculoskeletal treatment when appropriate.
This information is general and not a substitute for professional medical advice. Chiropractic care focuses on musculoskeletal health, and outcomes vary by individual. Always consult a qualified healthcare professional before making decisions about your health.
FAQs
Do I need imaging before spinal mobilisation?
Imaging isn’t always a must before spinal mobilisation. However, it becomes important when red flags are present, such as recent trauma, unexplained weight loss, or neurological symptoms. These could point to underlying issues that need further medical assessment. If you’re unsure or worried, it’s best to consult a qualified healthcare professional.
What symptoms indicate I should go to Emergency?
If you notice severe neurological issues, sudden weakness, loss of bladder or bowel control, or signs of infection or a fracture, seek emergency medical help immediately. These symptoms could indicate serious underlying conditions that need urgent attention.
What should I tell my practitioner before treatment?
Before starting treatment, make sure to tell your practitioner about any warning signs or symptoms you’re experiencing. This includes things like recent injuries, unexpected weight loss, fever, numbness, weakness, trouble walking, or issues with your bowel or bladder. These symptoms could point to serious health concerns that need medical attention. By sharing this information, you help ensure your safety and allow your practitioner to provide the right care for your needs.