
When dealing with neck and back pain, how do you know if your treatment is working? Manual therapy, provided by a chiropractor in Sydney, exercise therapy, and medication each define "success" differently. Manual therapy uses hands-on techniques and evaluates both patient feedback (like pain levels and daily function) and physical tests (like range of motion). Exercise therapy focuses on strength and movement improvements, while medication prioritises pain relief. Each method has its own tools to track progress, such as the Visual Analogue Scale (VAS), Oswestry Disability Index (ODI), and physical performance tests.
Key findings:
- Manual therapy: 68.3% recovery rate in a 7-week study, combining subjective and physical measures.
- Exercise therapy: 50.8% recovery, focusing on active strength and mobility.
- Medication: 35.9% recovery, centred on pain reduction, with higher reliance on painkillers.
Tracking progress is about matching tools to treatment goals. For example, manual therapy combines patient-reported outcomes with measurable physical changes, while medication primarily tracks pain reduction. Choosing the right method depends on what matters most to you – pain relief, mobility, or long-term strength.
Quick Comparison Table:
| Method | Focus | Common Tools | Success Rate (7 weeks) |
|---|---|---|---|
| Manual Therapy | Joint mobility, pain, function | VAS, ODI, range of motion tests | 68.3% |
| Exercise Therapy | Strength, endurance | VAS, ODI, strength/balance metrics | 50.8% |
| Medication | Pain relief | VAS, pain diaries, analgesic use | 35.9% |
Each approach works differently, so understanding their strengths helps you make informed decisions about your care.
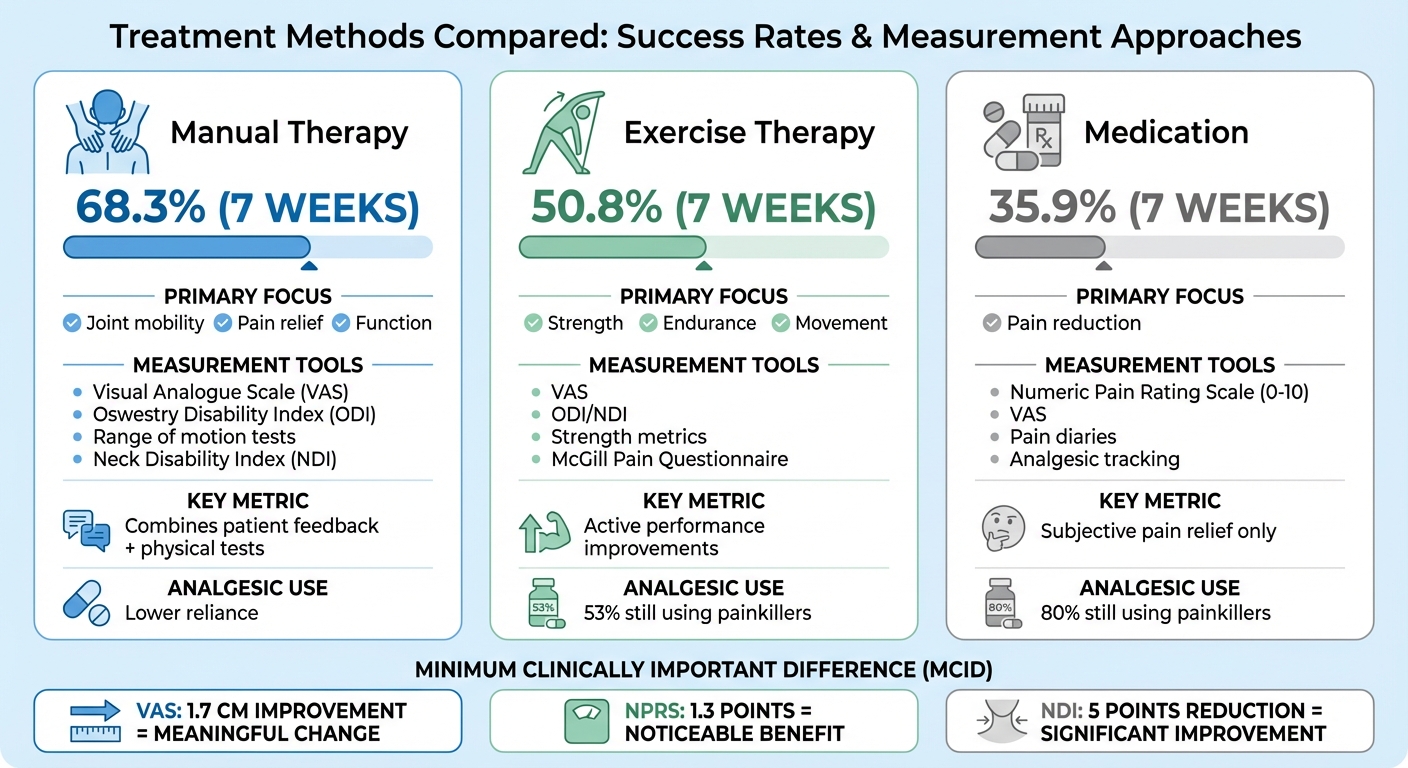
Manual Therapy vs Exercise vs Medication: Success Rates and Measurement Tools Comparison
Control Yourself podcast – Episode 26 Outcome Measures in Manual Therapy
sbb-itb-585d67d
How Manual Therapy Tracks Treatment Results
In manual therapy, practitioners use a mix of patient feedback and physical performance tests to evaluate treatment outcomes. Unlike medication-based treatments that often emphasise pain relief alone, manual therapy takes a broader approach, combining subjective experiences with measurable physical improvements.
Patient-reported outcome measures (PROs) capture how patients feel – covering pain levels, daily activity challenges, and overall progress. On the other hand, performance-based outcomes (PerfOs) provide objective data, such as range of motion or balance. Interestingly, these two measures don’t always match up. For instance, a patient might feel much better even if their physical performance shows only slight improvement, or the reverse might occur. This dual approach ensures a more comprehensive understanding of treatment effectiveness.
Patient-Reported Measurement Tools
To gauge how pain and dysfunction affect daily life, practitioners often turn to validated questionnaires. Tools like the Visual Analogue Scale (VAS) ask patients to rate their pain intensity on a numeric scale. Meanwhile, the Neck Disability Index (NDI) and Oswestry Disability Index (ODI) focus on how symptoms impact daily tasks, such as sleeping or lifting objects.
Another widely used tool is the perceived recovery scale, a six-point measure ranging from "much worse" to "completely recovered." Research published in the Annals of Internal Medicine highlights this scale as particularly effective because it combines pain, disability, and patient satisfaction into a single measure. For the NDI, a reduction of at least 5 points is considered a meaningful improvement.
After collecting these subjective insights, practitioners often turn to physical performance tests for more objective data.
Physical Performance Tests
Physical tests provide measurable insights into a patient’s functional abilities. For example, the Cybex Electronic Digital Inclinometer measures spinal motion in degrees, allowing practitioners to track changes in cervical or lumbar range of motion. The Berg Balance Scale evaluates stability and postural control, with a 4 to 7-point increase typically signalling improvement.
These tests not only offer clear benchmarks for tracking progress but also help with documentation for insurers. According to the American Physical Therapy Association, standardised outcome measures create a shared framework for identifying the most effective clinical practices, making them an essential part of modern manual therapy.
How Other Treatment Methods Measure Success
When it comes to measuring success, different treatment methods bring their own set of tools and priorities. While manual therapy combines patient feedback with performance metrics, other approaches – like exercise therapy, physical therapy modalities, and medication-based treatments – use measures tailored to their specific goals. These methods may share some overlap, but their focus often shifts depending on whether the aim is to build strength, alleviate pain, or restore function. Each approach adapts its metrics to address musculoskeletal issues in its own way.
Exercise Therapy and Physical Therapy Modalities
Exercise-based treatments focus heavily on active performance metrics in addition to standard pain and disability scales. Practitioners track progress in areas like strength, balance, coordination, and functional performance. Tools like the Visual Analogue Scale (VAS) and the McGill Pain Questionnaire, commonly used in manual therapy, are also applied here but with an emphasis on pain levels during movement. Disability indices, such as the Oswestry Disability Index (ODI) and Neck Disability Index (NDI), assess how symptoms affect daily activities.
A study conducted in the Netherlands involving 183 patients compared exercise-based physical therapy, manual therapy, and general practice care. The group receiving exercise therapy reported a 50.8% success rate after seven weeks, though 53% of participants were still relying on analgesics.
"Active exercise therapy involves participation by the patient and includes active exercises (to improve strength or range of motion), postural exercises, stretching, relaxation exercises, and functional exercises." – Annals of Internal Medicine
In addition to pain and disability metrics, physical therapists often monitor secondary outcomes. These include reduced reliance on painkillers and fewer work absences. Tools like the Euro Quality of Life (EQ-5D) self-rated health index offer a broader view of patient wellbeing, while digital inclinometers provide precise measurements of spinal mobility and range of motion.
Medication-Based Treatments
Medication-based treatments take a different approach, focusing almost entirely on subjective pain reduction. The Numeric Pain Rating Scale (0–10) is a key tool for tracking pain levels, often supported by the VAS and McGill Pain Questionnaire. Functional assessment tools like the ODI and NDI are sometimes used to evaluate whether medication helps patients manage daily activities. Additionally, 6-point ordinal transition scales allow patients to describe their status, ranging from "much worse" to "completely recovered."
Another important measure in this approach is the tracking of analgesic use through patient diaries. However, medication-based treatments often show lower success rates compared to physical interventions. In the same Netherlands trial, patients receiving care primarily based on medication and general practitioner advice had a success rate of 35.9% after seven weeks, with 80% still using painkillers. Notably, nine patients in this group reported worsening symptoms by the three-week mark, whereas no such cases were reported in the manual therapy group.
Because medication-based treatments focus narrowly on pain relief, they typically overlook physical performance metrics like range of motion – areas where exercise-based and manual therapies often show more tangible improvements.
Comparing Measurement Methods Across Treatments
When looking at different treatment methods side by side, it’s clear that while they share some measurement tools, their focus areas often differ significantly.
Shared Measurement Tools
Manual therapy, exercise therapy, and medication-based treatments all rely on several well-established tools to measure outcomes. Common examples include the Visual Analogue Scale (VAS), McGill Pain Questionnaire, Oswestry Disability Index (ODI), and Quebec Back Pain Disability Scale. These tools provide a way to compare results across treatments, even when the methods themselves are quite different.
In addition to these, secondary outcomes such as patient satisfaction, quality of life, and analgesic use are often evaluated. Interestingly, some research suggests that manual and exercise therapies may reduce the need for painkillers compared to ongoing general practitioner care. Still, while the tools are similar, each treatment type highlights different aspects of recovery.
Different Focus Areas
Each approach brings its own priorities to the table. Manual therapy tends to focus on immediate improvements in joint mobility and soft tissue function. This often involves physical assessments like palpation and range-of-motion tests. Exercise therapy, on the other hand, emphasises measurable progress in strength, endurance, and movement capabilities over time. Meanwhile, medication-based treatments zero in on pain relief and the reduction of analgesic use, rather than physical performance metrics.
Jan Lucas Hoving, PT, PhD, sheds light on the unique focus of manual therapy:
"Because perceived recovery combines other outcomes, such as pain, disability, and patient satisfaction, it may be the most responsive outcome measure [for manual therapy]."
These distinct priorities align with the core goals of each treatment. Manual therapy aims for quick, mechanical improvements that can offer immediate relief. Exercise therapy, however, is about building long-term resilience and physical strength. Pharmacological treatments focus on managing symptoms rapidly through chemical pathways, without necessarily addressing mobility or functional improvements. Understanding these differences helps clarify why recovery timelines and success rates vary, even when the same measurement tools are used.
Selecting Appropriate Measurement Tools for Musculoskeletal Care
Picking the right tools to measure outcomes in musculoskeletal care is crucial for tracking changes that genuinely impact a patient’s daily life. The Minimum Clinically Important Difference (MCID) plays a key role here, helping clinicians determine whether an improvement is not just statistically significant, but meaningful to the patient. For example, a 1.7 cm improvement on the Visual Analogue Scale (VAS) or a 1.3-point change on the Numerical Pain Rating Scale (NPRS) signals a difference that patients can actually feel.
Efficiency also matters. Quick and reliable tools, like a 6-point perceived recovery scale, can combine measures of pain, disability, and satisfaction without taking up too much time. On the other hand, more specific techniques, such as vertebral manipulation, often require multiple patient positions and lengthy evaluations. Dr Leonardo Costa highlights this difference:
"For specific vertebral manipulation, the therapist needs to perform several palpation tests that require different patient positioning. In non-specific manipulation, many of these procedures are unnecessary."
Patient perception is another factor that can influence results. For instance, some individuals interpret "0" on a pain scale as "manageable pain" rather than "no pain", which can skew outcomes. Additionally, patients with low baseline pain levels (e.g., below 3/10) may experience a "floor effect", where standard scales fail to capture meaningful improvement. To address this, combining patient-reported outcomes like the Oswestry Disability Index with objective measures, such as grip strength or range of motion, provides a more comprehensive view of progress.
The order in which measurements are taken also plays a role. Starting with subjective pain ratings, followed by physiological measures like blood pressure, and ending with physical performance tests (e.g., range of motion) can minimise the influence of one test on another. This structured approach supports the need for consistent and reliable methods that integrate various treatments into a cohesive framework for assessing patient outcomes.
Conclusion
Manual therapy and other treatment methods rely on well-established measurement tools like the VAS, NPRS, and Oswestry Disability Index to compare outcomes across different approaches. These tools help practitioners determine whether therapies such as manual techniques, exercise programs, or medications lead to meaningful progress.
To put it into perspective, a change of 1.7 cm on the VAS or 1.3 points on the NPRS often marks the Minimum Clinically Important Difference. This is the point where many patients notice improvements in their day-to-day activities. Without these benchmarks, there’s a risk of focusing on statistical changes that might not translate into noticeable benefits for patients.
By combining subjective feedback with objective testing, practitioners can gain a more comprehensive view of treatment outcomes. This blend helps address the limitations of relying on a single type of measurement and ensures a more complete evaluation.
Using validated tools also enhances communication about treatment options. When progress is demonstrated with reliable measures, it builds confidence in the chosen approach. Whether manual therapy is used on its own or alongside exercises and medications, consistent and objective tracking helps guide better decisions in musculoskeletal care.
This content is general in nature and should not replace professional medical advice.
Chiropractic care focuses on musculoskeletal health, and results vary between individuals.
Always consult a qualified healthcare professional before making health-related decisions.
FAQs
Which outcome measure matters most for my goal?
When determining the best way to measure outcomes, it all comes down to your specific goal. If you’re focusing on pain relief, research highlights that tracking pain intensity is a crucial indicator. Techniques like manual therapy and spinal manipulation have shown evidence of helping reduce pain levels.
On the other hand, if your aim is to enhance mobility or functional ability, tools like range of motion assessments or disability scales might be more fitting. Studies also point out that manual therapy can be effective in improving these aspects as well.
How much change is considered meaningful on pain scales?
A meaningful shift on pain scales is often linked to the minimum clinically important difference (MCID). This represents the smallest decrease in pain intensity that patients recognise as helpful. The specific MCID value can differ based on the treatment context and is frequently referenced in studies comparing manual therapy to other treatment methods.
Why can pain improve without better movement (or vice versa)?
Pain and movement don’t always go hand in hand when it comes to improvement. That’s because they’re influenced by different mechanisms within the musculoskeletal system. For instance, manual therapy techniques, such as joint mobilisation in chiropractic care, can help ease pain, even if your range of motion remains restricted. On the flip side, exercises or physical therapy might improve movement and stability without necessarily reducing pain right away. The results you experience often depend on the treatment method and the underlying issues at play.