
Scoliosis is a sideways curve in the spine, often developing during growth spurts in adolescents aged 10–13. It affects 1–5% of children in Australia, with girls being up to 10 times more likely to experience worsening curves. Early detection is crucial, with signs like uneven shoulders or a rib hump prompting diagnosis through the Adam’s Forward Bend Test and spinal X-rays.
Treatment depends on the curve’s severity (measured by the Cobb Angle) and the child’s growth stage (Risser grade). Options include:
- Observation: Monitoring mild curves (<20°) with regular check-ups.
- Bracing: For curves between 20–45°, braces prevent progression during growth. Types include rigid TLSO braces and more flexible designs.
- Physical Therapy: Methods like the Schroth exercises strengthen spinal support muscles and improve posture.
- Surgery: For severe curves (>40°), procedures like spinal fusion or vertebral body tethering may be required.
The right treatment is based on the curve’s size, growth potential, and the patient’s needs. Regular monitoring ensures timely adjustments to the care plan.
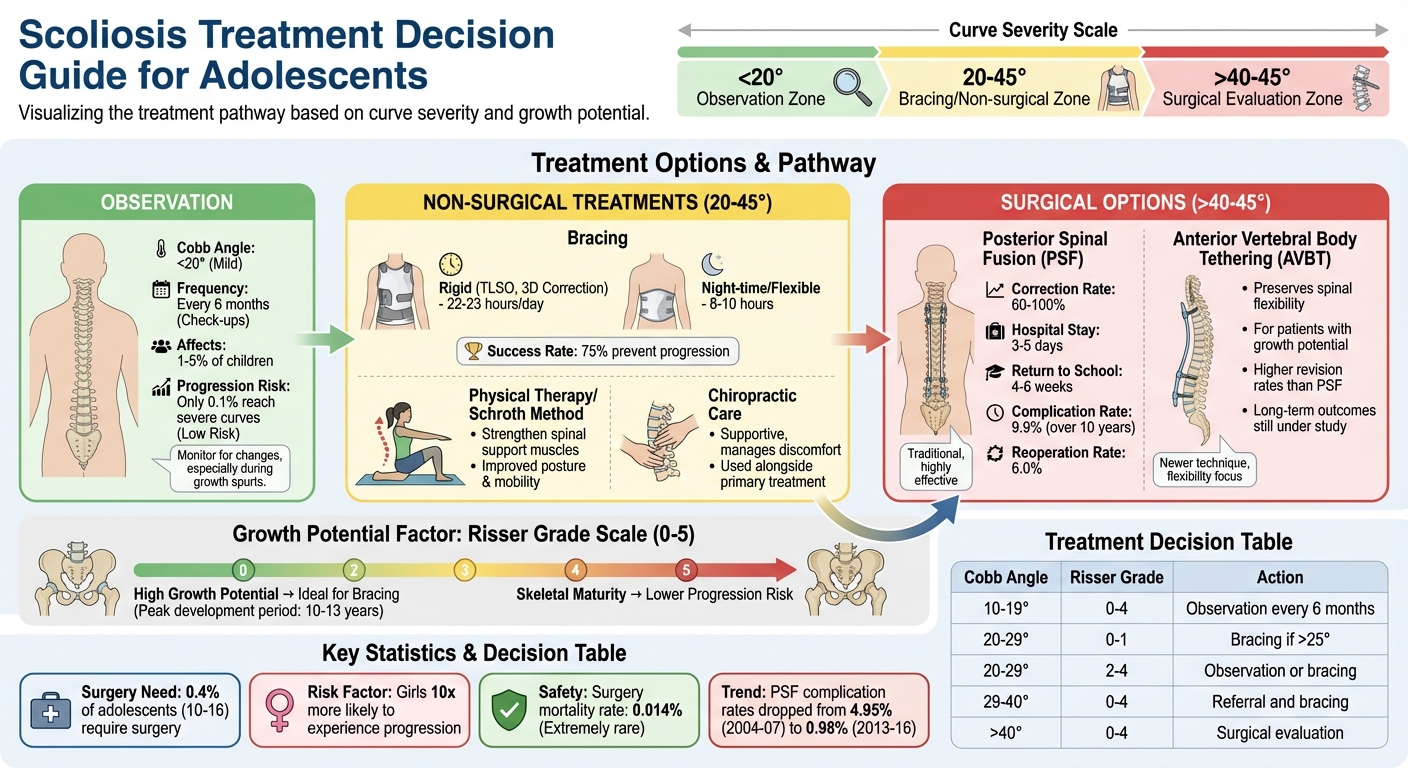
Scoliosis Treatment Options by Severity and Growth Stage
How To Treat Scoliosis In Teenagers?
sbb-itb-585d67d
Observation and Regular Monitoring for Mild Curves
For adolescents with mild scoliosis, healthcare providers rely on regular check-ups to keep an eye on the curve and see if it stays stable or worsens over time.
During these follow-ups, practitioners use tools like spine X-rays and the Adam’s Forward Bend Test to measure the Cobb Angle and assess for signs like rib prominence, uneven muscle tone, or visible curvature. Since females face a higher risk of curve progression, monitoring is especially important during growth phases. Once skeletal maturity is reached, the risk of progression usually stops, but until then, growth spurts can make the curve worse. Most curves that are simply observed stay under 40 degrees, with severe curves above this threshold affecting only about 0.1% of the population.
If the Cobb Angle starts to increase, treatments like bracing may come into play, as noticeable side effects tend to appear when the curve exceeds 40 degrees. Regular check-ups during growth are essential to catch any changes early, giving healthcare providers the chance to adjust the treatment plan as needed.
This observation-first approach ensures that treatment is only escalated when absolutely necessary. If progression is detected, additional options like bracing or physical therapy can be introduced to manage the condition effectively.
Non-Surgical Treatment Approaches
When an adolescent’s Cobb Angle falls between 20–45° and they are still growing, non-surgical treatments are often recommended. These methods aim to prevent the spinal curve from worsening during growth rather than correcting it. The earlier these treatments begin – before the spine reaches skeletal maturity – the better the chances of managing progression, as growth spurts pose the highest risk for curve worsening.
The three primary non-surgical options include bracing, physical therapy, and chiropractic care, each addressing scoliosis management in distinct ways. Research shows that bracing can reduce curve progression in up to 75% of cases, while physical therapy focuses on strengthening spinal support muscles. Chiropractic care, often used alongside other treatments, may enhance spinal mobility and alleviate musculoskeletal discomfort. Below, we’ll explore these approaches in greater detail.
It’s important to note that the success of these treatments hinges on consistency. For instance, braces must be worn for the prescribed hours daily to be effective, and physical therapy requires regular practice of exercises to maintain results.
Bracing: Types and Effectiveness
Bracing is designed to apply corrective pressure to the spine during growth, aiming to prevent the curve from worsening to the point where surgery might be needed. While bracing doesn’t straighten the spine, it often keeps the curve within six degrees of its original measurement. This treatment is typically prescribed for curves between 20–45° in adolescents still experiencing growth (Risser grade 0–2).
Most braces need to be worn for 22–23 hours daily, although newer designs have improved both effectiveness and comfort.
"The combination of improvements makes the brace more appealing to patients and more effective. When combined with the Schroth exercises, kids feel more active in their own care."
- Dr Jennifer Winell, Attending Surgeon at Children’s Hospital of Philadelphia
| Brace Type | Wear Time | Mechanism | Advantages | Disadvantages |
|---|---|---|---|---|
| TLSO (Rigid) | 22–23 hours/day | Applies side-to-side pressure to halt curve progression | High success rate (75%) | Can be bulky, restricts movement, may weaken muscles |
| Night-time Brace | 8–10 hours (overnight) | Corrects the curve while lying down | Easier compliance; doesn’t interfere with daily life | Not suitable for all curve types or magnitudes |
| 3D Correction Brace | Daytime/Full-time | Offers three-dimensional correction with lighter, thinner material | Easier to use; less heat retention | May not suit all curve patterns |
| Flexible/Soft Brace | Varies | Uses soft straps to support the middle or upper back | Comfortable; allows sports participation | Provides less rigid support; best for single curves |
Adherence to wear time is critical for success. Adolescents who wear their brace for more than 16 hours daily are far less likely to experience curve progression.
Physical Therapy and the Schroth Method
Physical therapy plays a key role in strengthening the muscles that support the spine, improving posture, and addressing compensatory movements. The Schroth Method, a specialised approach within physical therapy, uses tailored exercises to de-rotate, elongate, and stabilise the spine. These exercises incorporate targeted breathing techniques and postural corrections.
Physical therapy is often paired with bracing to combat muscle weakness that may result from brace use. While these exercises don’t typically alter the spinal curve itself, they can reduce discomfort, improve mobility, and enhance overall function.
Chiropractic Care for Spinal Mobility and Comfort
Chiropractic care is sometimes used as a supportive method to alleviate discomfort and improve spinal mobility in adolescents with scoliosis. Treatments may include gentle spinal manipulation, soft tissue therapies, and advice on posture and ergonomics. While chiropractic care doesn’t prevent curve progression, it can help manage back pain and movement restrictions when used alongside other treatments.
For some adolescents, scoliosis may also cause postural changes like muscle tension or leg length differences. In these cases, chiropractic care can improve biomechanics and provide relief, especially when combined with physical therapy.
For families in Bondi Junction, Dr Steve offers a gentle, nervous-system-focused approach to managing musculoskeletal concerns. While considered safe when performed by a qualified chiropractor, this care should always be coordinated with the primary scoliosis treatment plan.
Surgical Options for Severe Scoliosis
When less invasive treatments fail to stop the progression of scoliosis, surgical options become the next step. For adolescents, surgery is often considered when the spinal curve exceeds 40–45° or progresses quickly despite bracing. Around 0.4% of adolescents aged 10–16 require surgery to address severe scoliosis. Factors like skeletal maturity (assessed using the Risser grade), age, respiratory issues, and rib deformities also play a role in determining the need for surgery.
The main goals of surgery are to stop the curve from worsening and to reduce its severity. While it cannot make the spine perfectly straight, it can significantly improve alignment. There are two primary surgical approaches, each with distinct methods: one involves permanently fusing the vertebrae, while the other uses the patient’s growth potential to guide correction over time.
Posterior Spinal Fusion
Posterior spinal fusion (PSF) is the most commonly performed surgery for severe scoliosis. The procedure involves an incision along the back, where metal rods, screws, and hooks are used to hold the spine in a corrected position. Bone grafts – either from the patient (autograft) or a donor (allograft) – are placed between the vertebrae, which eventually fuse into one solid bone over 6 to 12 months.
This method achieves a correction of 60% to 100% of the curve. Hospital stays typically last 3 to 5 days, with patients returning to school in 4 to 6 weeks and resuming full activities within 6 months. Advances in technology, like intraoperative CT navigation, have improved screw placement accuracy and reduced the risk of nerve injury to between 0.7% and 1%.
"Our goal is always to provide a patient with the best chance not to need surgery, and in the event they do, our goal is to do the safest and best possible surgery, done right the first time."
- Dr Keith D. Baldwin, Attending Surgeon at Children’s Hospital of Philadelphia
While PSF is effective, it permanently limits motion in the fused sections of the spine. Over a 10-year period, the major complication rate is about 9.9%, with risks including surgical site infections, curve progression above or below the fused area (referred to as "adding-on"), and pulmonary issues. The reoperation rate is 6.0%, with complication rates decreasing significantly in recent years, from 4.95% in 2004–2007 to 0.98% in 2013–2016.
Anterior Vertebral Body Tethering
Anterior vertebral body tethering (AVBT) takes a different approach, aiming to preserve spinal flexibility. This newer, fusionless technique is designed for adolescents who still have growth potential. Surgeons place screws on the outer, convex side of the curve through a minimally invasive thoracoscopic approach. A flexible cord connects the screws and is tightened to create tension, which helps guide the spine to straighten as the patient grows.
The main advantage of AVBT is that it allows for continued spinal growth and retains flexibility. However, it’s a more complex procedure and has higher revision and complication rates compared to PSF, especially within three years of surgery. Common issues include tether breakage and overcorrection. Long-term outcomes are still under study.
"While a potential fusionless treatment for adolescent idiopathic scoliosis merits excitement, clinicians should consider AVBT with caution."
- Dr Patrick J. Cahill, Children’s Hospital of Philadelphia
| Feature | Posterior Spinal Fusion (PSF) | Anterior Vertebral Body Tethering (AVBT) |
|---|---|---|
| Approach | Incision from the back | Thoracoscopic (side/front) |
| Primary Goal | Permanent vertebrae fusion | Growth modulation without fusion |
| Implant System | Rigid rods and screws | Flexible cord (tether) and screws |
| Spinal Mobility | Motion loss in fused segments | Preserves flexibility |
| Reliability | Highly predictable | Newer, with higher revision rates |
| Ideal Candidate | Curves >50°; skeletally mature | Adolescents with growth potential |
| Correction Rate | 60–100% | Still under evaluation |
Monitoring over the long term (10+ years) is crucial to detect potential complications. Deaths from scoliosis surgery are exceedingly rare, occurring in only about 0.014% of cases.
How to Choose the Right Treatment
Selecting the most suitable treatment for adolescent scoliosis hinges on understanding a few key factors unique to each patient. Whether the path forward involves observation, bracing, or surgery, decisions are typically shaped by the severity of the spinal curve (measured as the Cobb angle), the patient’s growth potential, and their lifestyle needs.
The Cobb angle serves as a critical starting point. For curves under 20°, periodic observation is often sufficient. When the angle falls between 20° and 45°, bracing is commonly recommended. For curves exceeding 40°, a surgical evaluation is usually advised.
Growth potential is another essential consideration. To gauge this, clinicians rely on the Risser grade, which ranges from 0 to 5. Adolescents with a Risser grade of 0 to 2 have significant growth remaining, making them ideal candidates for bracing. On the other hand, once skeletal maturity is reached – typically Risser grade 4 for females and grade 5 for males – the likelihood of curve progression drops significantly.
Here’s a quick overview of treatment recommendations based on Cobb angle and Risser grade:
| Cobb Angle (degrees) | Risser Grade | Recommended Action |
|---|---|---|
| 10 to 19 | 0 to 4 | Observation; radiography every 6 months |
| 20 to 29 | 0 to 1 | Referral; bracing if curve exceeds 25° |
| 20 to 29 | 2 to 4 | Observation or bracing (Risser 4 often managed with observation) |
| 29 to 40 | 0 to 4 | Referral and bracing |
| > 40 | 0 to 4 | Surgical evaluation recommended |
Lifestyle considerations also play a role in shaping treatment plans. For instance, rigid braces, which typically need to be worn for 22 to 23 hours a day, can be removed temporarily for activities like sports or bathing. Flexible braces, however, may be a better choice for active adolescents with single curves, as they allow greater mobility. If surgery becomes necessary, families often face a choice between posterior spinal fusion, which offers predictable outcomes, and fusionless options like vertebral body tethering. While the latter preserves spinal flexibility, it does come with a higher likelihood of requiring revisions. Additionally, it’s worth noting that females are more prone to curve progression than males.
Conclusion
Adolescent scoliosis care involves a range of treatments tailored to the curve’s severity and the individual’s growth stage. For curves under 20°, regular observation is often sufficient to monitor changes during growth. If the curve progresses beyond this, bracing can be used to slow or halt further development, though its success depends heavily on consistent use. In severe cases where curves exceed 40°, surgical options like posterior spinal fusion or vertebral body tethering may be necessary to avoid long-term complications.
Treatment decisions are guided by factors such as the Cobb angle, growth potential (evaluated using the Risser scale), and the patient’s specific needs. Ongoing monitoring is essential, as the risk of progression varies from case to case.
Healthcare professionals rely on standard diagnostic tools to adjust treatment as the adolescent grows and the spinal curve changes. Whether through observation, bracing, or surgery, the approach is adapted to meet the patient’s needs over time.
Successful management of scoliosis depends on consistent adherence to the treatment plan, regular check-ups during growth periods, and maintaining open communication with healthcare providers. Aligning the treatment approach with the curve’s severity and growth potential can help manage scoliosis effectively.
This content is for informational purposes only and not a substitute for professional medical advice. Chiropractic care focuses on musculoskeletal health, and outcomes can vary. Always consult a qualified healthcare professional before making health-related decisions.
FAQs
How quickly can scoliosis worsen during puberty?
Scoliosis tends to worsen during puberty, particularly while growth is still happening. Adolescents with spinal curves measuring 25 degrees or more face a greater likelihood of progression. Notably, females are up to 10 times more likely than males to experience a significant increase in the curve. Growth spurts play a major role in how quickly the condition may advance.
How can you tell if a brace is effective?
The success of a brace is tracked through regular follow-up appointments, which often include X-rays to assess the Cobb Angle. This measurement helps gauge whether the spinal curve is staying stable or worsening as the individual grows. Monitoring these changes over time ensures the brace is meeting treatment objectives.
Can sports and exercise still be done with scoliosis?
Many individuals with scoliosis can still enjoy sports and exercise, as long as they follow guidance tailored to their condition. For those with mild scoliosis, staying active is often not only safe but can also promote better musculoskeletal health. That said, it’s crucial to check in with a doctor or physiotherapist to ensure chosen activities are appropriate and won’t lead to discomfort or aggravate the condition.



